“three cytokine levels, namely the IFN-γ,
MIG and IFN-α2 … These cytokine
levels at the baseline could improve the prediction of the bumetanide
responders”
“… cytokines had a potential to construct a
blood signature for predicting and monitoring the bumetanide treatment in young
children with ASD.”
“a significant part of the clinical
heterogeneity in the treatment effect of bumetanide for ASD is associated with
the differences in the immune system of patients”
Autism is a
very heterogeneous family of conditions and this is a big part of the reason
why all clinical trials to date have failed.
Ideally, there would be a diagnostic test to identify which person will
respond to which therapy. Then you can
have a successful clinical trial, because you are only including people likely
to respond.
Researchers
from China have just published their results that suggest that a blood test
measuring three inflammatory markers can predict who will respond to
bumetanide. This is good news and where
it is coming from is also very notable.
Autism
research has been very fragmented, some of it is very sophisticated and
insightful but much is very amateur and some is quite trivial. There is usually a real lack of common sense
among these people and no sense of urgency whatsoever.
China is a
very organised country; plans are made and then they are implemented. Forget political correctness.
This kind of
approach is what is required to move along with autism treatment.
In addition,
there is also another new study from China, this time on the microbiota in
autism that compared those with and without GI problems (it found it is equally
disturbed in both groups). Hopefully, that Chinese group will do the next
common sense step and compare the microbiota of autistic people with and
without restrictive diets. To what extent to people give themselves a
microbiota problem through poor diet.
Disentangling the relationship of gut microbiota,
functional gastrointestinal disorders and autism: a case–control study on
prepubertal Chinese boys
The altered gastrointestinal microbiota composition in ASD appeared to be independent of comorbid functional gastrointestinal disorder
The
bumetanide researchers are from Fudan
University in Shanghai, one of the 3 ultra-selective Chinese Universities
alongside Tsinghua University and Peking University in Beijing.
The paper, not surprisingly, may look complicated,
but there are a great deal of interesting things in it.
In their words:-
An immuno-behavioural covariation was
identified between symptom improvements in the Childhood Autism Rating Scale
(CARS) and the cytokine changes among interferon (IFN)-γ, monokine
induced by gamma interferon and IFN-α2. Using this covariation, three
groups with distinct response patterns to bumetanide were detected
The three groups were: best
responders, least responders and medium responders.
It should be noted that the dosage
used in their trials was 0.5mg of bumetanide twice a day.
Chinese children tend to be smaller
than Western children and this might help explain why the results were more
positive than in Servier’s failed phase 3 clinical trial in Europe. I also
imagine the Chinese children were more severely autistic than the European
group.
The dosage used is selected to
minimize the diuresis rather than to maximize the impact on the autism. This is
understandable, but I think it is a mistake.
Bumetanide, a drug being studied in autism
spectrum disorder (ASD) may act to restore gamma-aminobutyric acid (GABA) function,
which may be modulated by the immune system. However, the interaction between
bumetanide and the immune system remains unclear. Seventy-nine children with
ASD were analysed from a longitudinal sample for a 3-month treatment of
bumetanide. The covariation between symptom improvements and cytokine changes
was calculated and validated by sparse canonical correlation analysis. Response
patterns to bumetanide were revealed by clustering analysis. Five classifiers
were used to test whether including the baseline information of cytokines could
improve the prediction of the response patterns using an independent test
sample. An
immuno-behavioural covariation was identified between symptom improvements in
the Childhood Autism Rating Scale (CARS) and the cytokine changes among
interferon (IFN)-γ, monokine induced by gamma interferon and IFN-α2.
Using this covariation, three groups with distinct response patterns to
bumetanide were detected, including the best (21.5%, n = 17;
Hedge’s g of improvement in CARS = 2.16), the least (22.8%, n = 18; g = 1.02)
and the medium (55.7%, n = 44; g = 1.42) responding
groups. Including the cytokine levels significantly improved the prediction of
the best responding group before treatment (the best area under the curve,
AUC = 0.832) compared with the model without the cytokine levels (95%
confidence interval of the improvement in AUC was [0.287, 0.319]). Cytokine measurements can help
in identifying possible responders to bumetanide in ASD children, suggesting
that immune responses may interact with the mechanism of action of bumetanide
to enhance the GABA function in ASD.
The use of bumetanide as a potential drug to improve
symptoms in ASD is based on a hypothesised pathoetiology of ASD, namely the
delayed developmental switch of the gamma-aminobutyric acid (GABA) functioning
from excitatory to inhibitory [10,11,12]. In the valproate and fragile X rodent models of
autism, this GABA-switch can be facilitated by the reduction of intracellular
chloride concentration, which is mediated by a sequential expression of the
main chloride transporters, such as the potassium (K)-Cl co-transporters 2
(KCC2) and the importer Na-K-Cl cotransporter 1 (NKCC1) [12]. Therefore, bumetanide as an NKCC1 inhibitor has
been tested for its ability to restore GABA function in ASD [5,6,7, 13, 14]. However, these transporters can also be influenced by other molecules,
such as cytokines, which are a number of small cell-signalling proteins closely
interacting with each other to modulate the immune reactions. The
cytokines have been implicated not only in brain development [15], but also in GABAergic transmission [16,17,18]. It has been reported that the interferon (IFN)-γ can
decrease the levels of NKCC1 and the α-subunit of Na+-K+-ATPase,
contributing to the restore of inhibitory GABA function [16]. In mice subjected to maternal deprivation, the
interleukin (IL)-1 has also been found to reduce the expression of KCC2,
delaying the developmental switch of the GABA function and thereby possibly
contributing to the pathophysiology of developmental disorders such as ASD [17, 18]. Therefore, a question naturally arises that
whether the treatment effect of bumetanide for ASD can be affected by the
immune responses in the patients.
Indeed, compared with healthy controls, changes of
the cytokine levels have already been reported in patients with ASD [19,20,21,22]. Recent meta-analyses showed that the levels of
anti-inflammatory cytokines IL-10 and IL-1 receptor antagonist (Ra) were
decreased [20], while proinflammatory cytokines IL-1β,
IL-6 and anti-inflammatory cytokines IL-4, IL-13 were elevated in blood of
patients with ASD [21]. The levels of IFN-γ, IL-6, tumour necrosis
factor (TNF)-α, granulocyte-macrophage colony-stimulating factor
(GM-CSF) and IL-8 were observed to be elevated [22] in postmortem brain tissues of ASD patients, and
increased level of IFN-γ, monocyte chemotactic protein (MCP)-1, IL-8,
leukaemia inhibitory factor (LIF) and interferon-gamma inducible protein
(IP)-10 were found in another study [23]. These widely spread changes suggest that the
cytokine signalling in ASD may be better characterised by multivariate patterns
of cytokines. In literatures, many associations had been reported between the
levels of cytokines (e.g., MCP-1, IL-1β, IL-4, IL-6, etc.) and both core
symptoms and adaptive functions in children with ASD [24,25,26]. Therefore, it has been suggested that cytokines may be used as
biomarkers to identify different subsets within ASD. In each of these subsets
the patients with ASD may share a commonly immune-related pathoetiology and
therefore may have similar profiles of response to treatment [27].
Based on
these previous findings, we analysed data acquired through the Shanghai Xinhua
ASD registry, China, that began in 2016 to test the hypothesis that the immune
activity of patients might help to identify the best responders to bumetanide
in ASD.
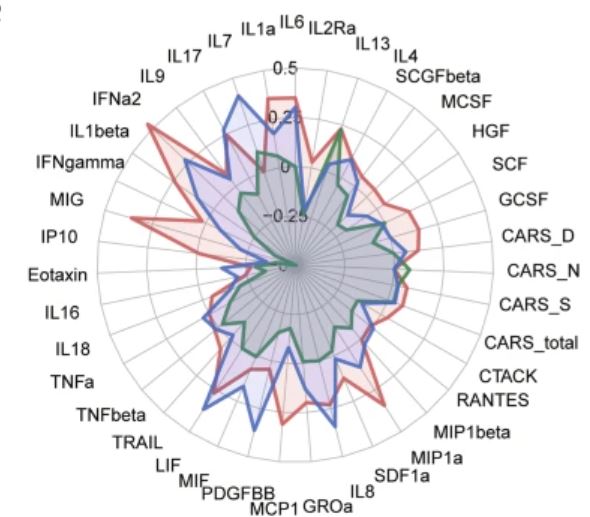
Between May 1st, 2018, to April 30th, 2019, a total of 90 ASD children, aged 3–10 years old, under a 3-month stable treatment of bumetanide without behavioural interventions and any concomitant psychoactive medications had both blood draws and behavioural assessments. Among these patients, 11 of them were further excluded due to the lack of the follow-up data at month 3. A group of 37 children, under 3-month stable treatment of placebo without behavioural interventions and any concomitant psychoactive medications had both blood draws and behavioural assessments. Therefore, the current analysis used a subsample of 116 young children with ASD, whose blood samples were available both before and after the treatment. The blood samples were sent in three batches (Discovery Set: n = 37 on December 4, 2019; Validation Set: n = 42 on May 22, 2019; and Control Set: n = 37 on January 5, 2022) to measure the serum levels of 48 cytokines for the immune response (Table S1), and the clinical symptoms were assessed using CARS, ADOS and the Social Responsiveness Scale (SRS).
In this study, we observed a
significant improvement of clinical symptoms with bumetanide treatment in
children with ASD, and such improvement was associated with a pattern of
changes in three cytokine levels, namely the IFN-γ, MIG and IFN-α2
(r = 0.459 in the Discovery Set and r = 0.316 in the
Validation Set). These cytokine levels at the baseline could improve the
prediction of the bumetanide responders compared with using the behavioural
assessments alone, and the best predictor achieved an AUC of 0.83 in the
independent test data set (Table S8).
The implications of these findings may be twofold: (1) a significant part of
the clinical heterogeneity in the treatment effect of bumetanide for ASD is
associated with the differences in the immune system of patients, and (2) the
component score of cytokines had a potential to construct a blood signature for
predicting and monitoring the bumetanide treatment in young children with ASD.
Following the protocols of previous studies [8], bumetanide treatment consisted of two 0.5 mg tablets
per day for three months, given at 8:00 a.m. and 4:00 p.m. The tablet size is
8 mm diameter x 2 mm thickness, which is quite small. Each time, the patient
took half of a tablet, which was not difficult for most of the patients.
However, the careers were recommended to grind the half-tablet into powder and
give the powder in water, if necessary. Possible side effects were closely
monitored during the treatment. Blood parameters (serum potassium and uric
acid) were monitored via laboratory tests (Table S2) and symptoms (thirst, diuresis, nausea, vomiting,
diarrhoea, constipation, rash, palpitation, headache, dizziness, shortness of
breath, and any other self-reported symptoms) were telephone interviewed
(Table S3), and both of them were reported to the research
team by telephone at 1 week and 1 month after the initiation of treatment and
at the end of the treatment period. The cytokine levels of the children with gastrointestinal problems were
compared with those without such problems (Table S4).
The supplemental table S4 shows that GI
problems had no effect on cytokine levels.
Changes
after the administration of bumetanide
Seventy-nine patients were treated with bumetanide
for 3 months, and the CARS total score decreased after the treatment (effect
size Cohen’s d = 1.26, t78 = 11.21, p < 0.001).
The treatment effect showed no difference between the Discovery Set and the
Validation Set (ΔCARS_total: mean(±SD): 1.54 (±1.40) vs. 1.90 (±1.34)). Consistent to the previous
studies of the low-dose bumetanide for ASD, the side effects were rarely
reported (Tables S2 and S3). No significant difference in the cytokine levels
between the children with and without the gastrointestinal problems at the
baseline (Table S4). A
number of cytokine levels were changed significantly after the treatment of
bumetanide, but none of them was changed significantly after the treatment of
placebo (Table S6). No significant pairwise association could be
identified in the Discovery Set, the Validation Set and the Control Set among
four groups of variables, including the baseline CARS total score, the baseline
cytokine levels, the change of CARS total score, and the changes of cytokine
levels (Fig. S2).
In this study, we
observed a significant improvement of clinical symptoms with bumetanide
treatment in children with ASD, and such improvement was associated with a
pattern of changes in three cytokine levels, namely the IFN-γ, MIG and
IFN-α2 (r = 0.459 in the Discovery Set and r = 0.316
in the Validation Set). These cytokine levels at the baseline could improve the
prediction of the bumetanide responders compared with using the behavioural
assessments alone, and the best predictor achieved an AUC of 0.83 in the
independent test data set (Table S8). The implications of these findings may be twofold: (1) a significant
part of the clinical heterogeneity in the treatment effect of bumetanide for
ASD is associated with the differences in the immune system of patients, and
(2) the component score of cytokines had a potential to construct a blood
signature for predicting and monitoring the bumetanide treatment in young
children with ASD.
Accumulating
evidences support that IFN-γ can inhibit chloride secretion [38] and down-regulate both
the NKCC1 expression [16, 38] and the Na+-K+-ATPase
expression [16], which had been
implicated in the GABAergic dysfunction in ASD [10, 39].
The
cytokine-symptom association was identified in the changes after the treatment
of bumetanide but not before the treatment, suggesting that bumetanide might
interact with the cytokines and the changes of which contributed to the
treatment effect of bumetanide. Animal studies showed a rapid brain efflux of bumetanide,
but a number of clinical trials have shown a significant treatment effect for
neuropsychiatric disorders, including ASD, epilepsy and depression [41, 42]. These findings may suggest the
possible systemic effects of bumetanide as a neuromodulator for these
neuropsychiatric disorders. Considering its molecular structure, bumetanide has
been recently identified by an in vitro screen of small molecules that can act
as an anti-proinflammatory drug via interleukin inhibition [43]. This
anti-proinflammatory activity of bumetanide might alter the blood levels of
cytokines outside the brain-blood-barrier (BBB).
Our findings
may suggest that the identified canonical score of cytokines had a potential to
construct a blood signature for predicting and monitoring the bumetanide
treatment in young children with ASD. Accurately identifying patients who are
likely to respond positively to bumetanide can facilitate the precision
medicine for ASD. Our prediction model based on the cytokine levels before the
treatment may provide a potentially new tool for the precision medicine of
ASD.
In summary, we identified an association between the changes of
the cytokine levels and the improvements in symptoms after the bumetanide
treatment in young children with ASD, and found that the treatment effect of
bumetanide can be better characterised by an immuno-behavioural covariation.
This finding may provide new clinically important evidence supporting the
hypothesis that immune responses may interact with the mechanism of bumetanide
to restore the GABAergic function in ASD. This finding may also have relevance
for determining enriched samples of ASD children to participate in novel drug
treatment studies of drugs with a similar mode of action to bumetanide, but
with potentially greater efficacy and fewer side effects.
Conclusion
I think we can give the Shanghai
researchers 10 out of 10 for their paper.
Monty, aged 18 with ASD, has been to
Shanghai twice. It is a vast city, but well worth a visit. With the high speed
train network it is now very easy to travel around China, quite different to
when I visited as a teenager.
Hopefully the Chinese will continue in
their pursuit of precision medicine for autism. They do not have much
competition.
My perspective is a little different
because I know that a bumetanide responder can cease to be a responder when
affected by an inflammatory condition like allergy, which increases pro-inflammatory
cytokines like IL-6. This suggests that some people with elevated cytokines are
potential responders, you just have to use an anti-inflammatory therapy before
you start bumetanide therapy. The inflammatory cytokines shift the balance
between NKCC1 and KCC2 towards NKCC1 and so increasing intracellular
chloride. We also know that some people
need a dose higher than 0.5mg twice a day to see a large benefit; I have been
using 2mg once a day for several years.
The Chinese researchers have
established biomarkers for who is likely now to respond to bumetanide. This
certainly is a big step forward, if it can be replicated. This is not the same
as identifying who could respond to bumetanide, if their current inflammatory
condition was moderated. The levels of specific cytokines might indeed mark
someone as both a current non-responder, but also as a potential future
responder.
Autism is all about n=1, it is about
the exceptions being more important than the average.
Unlike the Shanghai researchers, I do not
really see Bumetanide as an anti-inflammatory therapy in my son’s Polypill, but
I do have therapies included that are.
Understanding inflammation will be a
key to treating autism using precision medicine. That is less simple that it sounds. When it
comes to preventing autism, inflammation in the mother is a key part of the
equation. This also gets complicated, maternal antibodies damage the brain of
the fetus, no genetic mutations were needed.
Wow! This is indeed huge news. Is this the first time researchers have found bio markers that correspond to responders in an autism treatment?
ReplyDeleteThere are biomarkers for some other therapies, but they are not 100% reliable.
DeleteBiomarkers should help clinical trials be successful enough to get drugs approved officially.
When it comes to actual treatment, they can be a guide rather than a guarantee. Still much better than nothing.
Hello, mr. Peter, (sorry for my English)
ReplyDeleteI read your blog for a few years and I am excited about your way of thinking and resolving problems which seem impossible to deal with.
I have a daugther with autistic spectrum age 7 years now and also came a long way through different kinds of treatments and behavioral therapies. Now she can speak our native language, read one or two sentencies in a row and can be engaged in different physical activity like swimming or hiking. But still we have a lot to do. Our main problem now (on my opinion) is hyperactivity, absent of concentration, hysterical behavior and big problems with shortterm memory. So it is hard to teach her some really new skill.
I was trying some medicines from your list and can`t say that it was great result but all time I am trying to recearch and look for new information to help my Veronika`s condition. These days I stumbled upon one intersting trial:
https://clinicaltrials.gov/ct2/show/NCT04644003?term=stp1&draw=2&rank=1
Did you see it? I want to ask your opinion about because you are the only person in the word which I can ask for such advise.
I can try this kind of treatment, because I think I can get that japanese medicine ibudilast, and I have some supply of bumetanide. My family lived in Ukraine, but we have been forced to move to Germany because of war and now I have problems here with finding proper school for Veronika, because of her language barrier and behavior problems. So I am looking for treatment to improve her condition and decrease hyperactiity for better integration here.
Dear Anatolii, my daighter has the same problem with focus as yours . Does your daughter have any signs of allergies? When we got those under control it went better for us (we used Mirokrom). Its on german amazon as Allergoval.
DeleteHello, Anatolii, if you are in Germany you have a big mud, you can buy Atarax 25mg, for us this medicine worked wonders, the agitation decreased drastically, it is more attentive and very concentrated, the vocabulary increased, it sleeps very well, you can try 10 mg in the morning and at noon and if he does not sleep 25 in the evening at bedtime .....
DeleteAnatolii read this:https://www.scitechnol.com/peer-review/h1r-antagonists-for-brain-inflammation-and-anxiety-targeted-treatment-for-autism-spectrum-disorders-VmP2.php?article_id=4284
DeleteI answered Anatolii directly offline. Since there are autoimmune and GI comorbidities, I suggested these need to be resolved first. I suggested Pentoxifylline as an alternative to Ibudilast. I suggested mast cell stabilizers and antihistamines. Due to possible hypoxia during birth I suggested Clemastine.
DeleteHi Peter, Thank you for always sharing your knowledge. My son will be 9 next month, he is on the spectrum. He is very hyperactive, he was recently prescribed low dose risperidone but I am not very comfortable with this. I have been following your blog for years and have tried a few times to comment but never seems to get through.
DeleteMy son has always had rashes/raised skin in his inner elbow and for a few months now small spots all over his body, which is very itchy. He is generally hyperactive, sometimes aggressive and he won't sit to learn. still struggling to learn to count from 1-10.
I want to try verapamil for mast cell activation. I also want to try atarax. Can I use both together?
We are on Bumetanide for the past 4 weeks as well.
What's your suggestion for learning disability therapy in addition to Bumetanide.
Olu, drug ineractions are shown on drugs.com. It has none listed for Verapamil plus Atarax.
DeleteIf your son has allergy, itching, dermatitis etc, this needs to be resolved to maximize the effect of bumetanide, assume he is a potential responder. Even if he is not a bumetanide responder, he will benefit from treating his auto-immune issues.
Some people get a pro-cognitive effect from low dose clonazepam, some from low dose roflumilast, some from pentoxifylline, some from Atorvastatin. It is down to trial and error.
The more aspects of your specific case of autism that you optimize the better the overall result will be.
Hello Peter, Thanks for your response, I have started him on Atarax and it seems to be having a calming effect, its just been a day and half.
DeleteDo you know how long one can stay on Atarax? And how long on Verapamil if he is a responder?
I will like to start with a trial of roflumilast, I have read your post about the dosage but I don't understand how to convert the tablets to mls using Alchohol. I will like if you can go over your explanation again.
Verapamil is mainly used as a long-term therapy as a calcium channel blocker and is well tolerated by most people. Atarax (hydroxyzine) is used for allergic skin conditions and for anxiety. Most people take antihistamine drugs just during the period for which there is an allergy present. Some people with mast cell conditions are permanently taking this kind of medication.
DeleteIf there is a clear benefit and there are no side effects, it would be reasonable to continue use. Discuss with your doctor.
Low dose Roflumilast was patented as a cognitive enhancer at a dose of 100 mcg in adults. Higher doses were not found to be effective.
My research suggested an even lower dose, which equates to 1 mcg per Kg.
Roflumilast (Daxas) is sold in 500mcg tablets as a treatment for COPD. It would be very hard to split into tiny pieces. The tablets are not water soluble, but they are soluble in alcohol.
If you take an old propolis tincture bottle with a pipette, you can repurpose it to make a roflumilast tincture. You just need to experiment to see how many drops contain the required amount of Roflumilast. If you add 3ml of your food grade alcohol to one 500 mcg tablet, you then see how many drops this gives from your pipette. If it was 60 drops, then you know that one drop contains 500/60 mcg = 8.3 mcg, If you want a dose of 40mcg you would want 5 drops.
Then you can make a more useful volume, say 5 pills in 15 ml of your alcohol. This would then be sufficient for 2 months. 40mcg x 60 = 2,400 mcg which is just about 5 tablets.
Many people use Pentoxifylline, and it has been in use for autism for nearly 50 years. This has multiple modes of action, one of which does overlap with Roflumilast. There is also Ibudilast which is extremely similar to Roflumilast and is now in a clinical trial for autism.
Pentoxifylline is very cheap and widely available. Ibudilast is mainly used in Japan as an asthma therapy. Daxas, at the full dosage, is expensive in the US, but more affordable elsewhere.
Hi, I want to send you to everyone who reads this blog, I have tried many drugs and supplements for our boy, and the best for us is verapamil, which we have been using for 2 years, but the star of all is Atarax.With each day administered, we see improvements, go for a drive, listen to loud music and have fewer preferences, before he made us change the radio channel, something has improved in sound, is calmer and happier, wants to bathe alone and without whims, he stays in his room only very little at all, and many improvements on the sociability side.Side effects, his nose is clogged, we do not know if he is from anthrax, 2 weeks ago he got a flu or cold, but I will let you know. Soon we will supplement with Galavit (someone from Ukraine had a big heart) and N-A-G. So try Atarax and you will see that I was right ..... the best for autism (autoimmune encephalitis) ....
DeleteThanks for your detail response Peter. I will work on it.
Delete@BuGA, how do you administer the Atarax, we give half of the 25mg morning and the other half in the evening.
Hi, we are taking atarax 25mg twice a day, our boy is 95kg and 1.82, height, 18 years old, so depending on his weight and the way he responds, at first he will make him a little more sleepy until he gets used to it. with the drug, if it is very hyper you can give it 3 times a day, 10mg * 3, or 10 * 10 * 25 in the evening, the higher dose in the evening if you do not sleep, we also administer l.plantarum v299 with 3 mg melatonin, and in 20 minutes he is at bedtime, and sleeps well ....
DeleteThe effect that Atarax will start to do its job better will be on the 4th day. if it goes well, there will be improvements from day to day.Inflammation in the brain probably decreases. Autism (autoimmune encephalitis) is an inflammation of the brain caused by an inflammation of an infection in the body (intestine or nose or throat) if we can stop this inflammation then the brain begins to return to normal
DeleteThank you Peter and Buga.
Delete@Peter have you tried Pentoxyfilline for Monty? If yes how do you schedule the polypill such that there is no interaction. Bumetanide/Pentoxyfilline/Verapamil and atarax. They all seem to have lowering blood pressure effect.
Yes, I did try Pentoxifylline, but it did not seem to provide a benefit. Bumetanide lowers blood pressure mainly by reducing the volume of fluids in your body. If you drink extra water to compensate, which is the natural reaction, there is no net fluid loss.
DeleteBut it is indeed wise to monitor blood pressure to be on the safe side.
The Verapamil dose in autism is quite a low dose and does not seem to cause a problem in most people. One problem that may occur in some people is inflammation of the gums, so good dental hygiene is advisable.
After nearly 10 years of therapy we have not had any worrying side effects. We even went to a pediatric cardiologist for an ultrasound examination, since as you have noted many of the autism drugs are re-purposed drugs for heart conditions.
Hello Peter, I have been doing some research on hyperactivity for my almost 9 year old ASD, I have read what you wrote about Verapamil and the comments about Atarax. Can I use both together?
ReplyDeleteThere are no listed interactions.
DeleteSomething in a similar direction has been recently found with Rett and IGF-1
ReplyDeletehttps://www.frontiersin.org/articles/10.3389/fnins.2022.868008/full
Most clinical studies are approached with a pharma industry mindset and the goal is just to prove the potential of a single compound or drug.
Yes, even within single gene autisms there are wide variations. This means that precision medicine has to be personal. As you suggest this does not fit with how medicine and its clinical trials work. It is evidence based medicine that assumes we are all the same. Even within Rett syndrome girls there are sub-groups and so no one size fits all solution
DeleteHi, Peter we want to give Denis n-acetyl-glucosamine (N-A-G), we saw that it has a lot of good anti-inflammatory and anti-anxiety effects.Do you think that the yeast in the system could increase, I have seen articles in which it is said that it kills candida or in some it increases it excessively, what do you think is worth a try, thanks Peter
ReplyDeleteDragos, the mouse research suggests NAG may increase oral candida. I think it would be wise that Denis swallows NAG as a capsule and not to take it as a powder.
DeleteIt is easy to see candida in the back of the mouth. If the NAG does cause candida then just stop your trial.
NAG has very interesting possible benefits, including on myelination. Some readers of this blog do take it. Nobody has mentioned any problems so far.
ReplyDeleteBUGA DRAGOS, may I ask how you discovered your son’s auto-immune encephalitis? Do you believe it causes his autistic features? It is interesting how many different ASD sub-types respond to Verapamil.
Hi Peter .Please do you know if Fluimicil is sold prescription free in Switzerland.I saw from your blog its manufactured there and a friend is presently there.I was wondering if I should get some as it seems to be the best.We started the Holland and Barrett brand on Thursday and stimming has reduced.Please is it sold as fluimicil there or what is the brand name. .Thank you Apinke
ReplyDeleteI just looked online. It does not need a prescription, but it is very expensive in Switzerland. Everything in Switzerland is over priced. Better find someone going to Poland.
DeleteI would just buy the capsules in the UK. The ones on Amazon are usually cheaper than Holland and Barrett
Thank you. I will stick to the UK then.My neighbours go to Poland a lot.Do you know what the Polish version is called.Thank you
DeleteIn Poland it is called Fluimucil Forte. 10 x 600mg effervescent tablets costs 13 zloty which is about £2.40.
DeleteHi, if you have a small child, you can do a set of tests and see if it is an autoimmune encephalitis. In Romania 14 years ago, when my child stopped talking and eating and playing, those at the hospital did tests and found only giardia and candida.If you can do more detailed tests, it would be good, not all children have autism, if my child received at the age of 4 a course of predinsolone (corticosteroids) we had another chance, but we only received risperidone, we are sure, after so many years that Denis does not have autism, it is just an encephalitis that appeared after the MMR vaccine . respond to verapamil because it is a dysfunction of the L-type calcium channel, it is an inflammation of the intestine, which along the way is affiliated with other infections that amplify inflammation of the brain.
ReplyDeleteSo interesting! Thank you!
Deletehttps://quillette.com/2022/01/21/autism-or-encephalitis/
ReplyDeleteBUGA DRAGOS does Denis have any hypoperfusion that you know of? I’m asking because my son does and in addition to Verapamil, he has responded to pentoxifylline. It improves language, memory, and even behavior.
ReplyDeleteHi Peter,
ReplyDeleteI wanted to give a quick update on my first “game changer” which might help families with children who have similar biological dysfunctions as me.
After trying many different interventions (NAC, ALA, PEA, Quercetin etc.), none of which had any effect, I realized I had an underlying allergic issue causing problems.
I started using a DAO supplement after every meal to break down the excess histamine. Like magic, my mood/sociability/focus all improved. It makes sense considering the H3 receptor mediates the release of dopamine, serotonin, acetylcholine etc.
I suspect I have a gene mutation preventing the DAO enzyme in my body from working properly. Since Monty (luckily) does not have this problem, DAO supplements are not part of your poly-pill. But other families who have children with allergy symptoms (itching, sneezing, irritability), who don’t respond to mast cell stabilizers, may want to consider DAO supplements.
Also Peter, have you kept a list of what supplements didn’t work with Monty? It might be interesting to see to help others out.
Thanks again for all your help. Your blog has helped me out tremendously.
Thank you for sharing your experience. My child has issues which I suspect are allergic and I have used DAO, however, I have given once daily, not after each meal. Do you think you are reacting to food and that is why you are taking the DAO with meals, or is it just to dose throughout the day?
DeleteHi,
DeleteI am taking the DAO with meals because I am reacting to the food.
Many foods have high histamine, which is the chemical that causes allergic symptoms. So if you have too much histamine you will experience anger, mood swings, itching, flushed skin etc.
In your stomach, DAO normally breaks down the histamine in the food you eat.
However, DAO can "stop working" and then it will not break down the histamine in the food. This extra histamine will enter your blood stream and then cause allergic symptoms - anger, flushed skin, anxiety etc.
I think my DAO "stopped working" because of stomach problems, so I take DAO supplements before every meal. Doing this reduces the histamine in my body, and makes me much more calm, happy, more clearheaded etc.
I have also been following this low-histamine food list which has also helped: https://www.histaminintoleranz.ch/downloads/SIGHI-Leaflet_HistamineEliminationDiet.pdf
Hi Peter. Thank you very much for your work. This blog is a beacon in the midst of the lack of information on autism. Regarding bumetanide, production was suspended in Brazil in 2018 and it is simply not available anymore. Is there a similar drug that can replace it satisfactorily? Grateful.
ReplyDeleteOne reader from Brazil told me that was able to acquire Bumetanide from a compounding pharmacy at a major hospital. This is the old kind of pharmacy where they have the bulk materials, rather than the ready made tablets in blister packs.
DeleteYou can acquire Bumetanide very easily in Mexico, as Miccil, if that is an option for you. In certain parts of Spain you can acquire Bumetanide, as Fordiuran, without prescription. Bumetanide is not available in Portugal.
I doubt you have connections to Egypt, but if you do, it is very cheap there and without prescription.
Some autism doctors seeing international patients seem to supply the drugs directly. Then it is just a questions of what happens at customs when the package reaches your country.
There are so-called international pharmacies in Germany and Switzerland, who specialize in acquiring drugs, often from other countries - even Japan, and then supplying you. You need a prescription and the risk of seizure at customs is on your side.
Great tips, thanks. If perhaps you remind whoever from Brazil it was and if you had any contact, please let me know. But you already have helped me a lot with this response. I will keep searching and I will get the medicine eventually, and I will let you know. Cheers. Wish you and Monty all the best.
DeleteHi Peter!
DeleteThanks to your advice, today I managed to have a box of Miccil in my hands, coming from Mexico from a father of an autistic boy to whom I had access. However, I would like to know your assessment of the evaluation procedure proposed by the neuropediatrician. She suggested taking a functioning scale (some kind of test administered by a psychologist) before and another after three months of use "to measure language gains", in her words. The indicated test is called IDADI (acronym in Portuguese for "multidimensional instrument for assessing child development"). I wonder if such a method will be effective, but in view of that I will first need to request a new shipment of pills to the acquaintance from Mexico, because he sent me only 20 pills and that would only take 20 days, and it took 40 days to get here on my Address in Brazil.
Taking the opportunity, I would like to ask you, how long, on average, can I see if my child responds to bumetanide? And which signs should I pay special attention to for such an assessment? Finally, with 20 pills of 1mg (for 20 days) could I start right now and personally see if my son responds, before I get a bigger supply, or does it take longer?
Thanks again for the help! You certainly hear this a lot, and you deserve it, you're special. Next time I'll try to create a login to stop commenting anonymously, my name is Hérson Cougo and I'm Bento's father, my little autistic today 5 years and a month. Thanks!
Herson, I would wait until you have another pack of Miccil before starting.
DeleteFor most responders it takes at least 10-15 days to see a benefit, but it can be longer.
The biggest effect is on cognition and the ability to learn new skills. The effect will be most obvious to any teachers or therapists who work with him 1:1. I do not think you need to use any formal assessment. Just do not tell people you are making a trial, wait until they come to you and ask why Bento has suddenly changed.
Yesterday I visited one of the doctors who conducted the phase 3 Bumetanide trial in one of the selected hospitals. I wanted to know more about the practicalities of treating with Bumetanide. I was lucky and found a kind and helpful doctor.
ReplyDeleteThe doctor told me:
There was CARS improvement but there was not a large difference with the placebo.
The Placebo effect could be very significant in the trial as there are no treatment alternatives for the families
CARS might not be the right scale.
The five patients who were on Bumetanide improved in hyperactivity and learning skills.
The families of these five patients decided to continue with the Bumentanide trial.
Once Bumetanide was discontinued for legal reasons, these 5 patients worsened very significantly. One of them had an accident due to hyperactivity.
These Bumetanide patients enjoyed their ever-best school year while on Bumetanide.
The placebo was another diuretic.
My conclusions are:
- Bumetanide might work for the NKCC1 blockage but this does not necessarily exclude additional benefits.
- Time ago I used to have a Chinese Gua Sha massage on my back. The Gua Shar massage had a powerful anti-inflammatory effect but also some diuretic action.
- The mental improvement effect after Gua Sha massage was incredible. So I was used to having a Gua Sha massage before every important meeting or event.
- I was suspicious if the placebo diuretic might also help the kids somehow. This is what I found at first sight:
Furosemide exhibited an anti-inflammatory effect through the inhibition of production and release of cytokines interleukin (IL)-6, IL-8, and tumour necrosis factor-alpha from peripheral mononuclear cells, which may have a beneficial effect on local inflamed tissue imbalance in the ratio of different cytokines, thus improving the sensitivity of target cells to endogenous glucocorticosteroids.
https://pubmed.ncbi.nlm.nih.gov/12115021/
- I never found a clear explanation why Gua Sha had such an anti-inflammatory and diuretic effect. The Chinese massagist used to tell me that I had stagnant water. The effect on anxiety, and mental clarity,... was striking.
- I have a box of Bumetanide next to me. I Definitely will give it a try as soon as I feel contracted, inflamed and mentally foggy. It might save me a visit to the Chinese massagist.
Hi Peter,
ReplyDeleteHere is a interesting article on Bumetanide and Gaba receptor. It appears there was also a case study of autistic children and flumazenil in the 90s that showed a positive effect as well. The thing that intrigued me the most is how it counteracts LPS.
https://pubmed.ncbi.nlm.nih.gov/34004209/
Stephen
Thanks
DeleteArticle on LPS causing neuroinflammation.
ReplyDeletehttps://jneuroinflammation.biomedcentral.com/articles/10.1186/s12974-019-1564-7#:~:text=Endotoxin%20is%20a%20lipopolysaccharide%20(LPS,other%20tissue%20during%20bacterial%20infection.